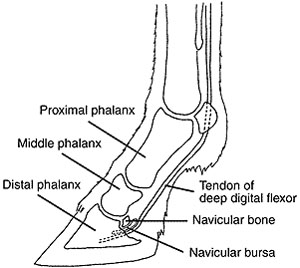
Navicular disease often begins as an inflammation of the bursa between the deep digital flexor tendon and the navicular bone of the foot (Figure 1).
While the joint surfaces of the phalanges may not be affected, the tendon adjacent to the bursa may he progressively destroyed with eventual rupture. This tendon is very important because it flexes the joints of the foot; that is, it moves the toe down and back. Horses with faulty conformation of the forelimb are more likely to develop navicular disease. Racing, cutting and roping horses have a higher incidence of navicular disease than pleasure horses. It is one of the most common causes of lameness in horses and usually affects both forefeet. However, one foot may have more extensive damage than the other.
When the foot is placed upon the ground, the weight forces the navicular bone back against the tendon. Horses with small feet have less area over which to distribute concussion and weight; therefore, more pressure is placed upon the navicular bone.
Signs of navicular disease
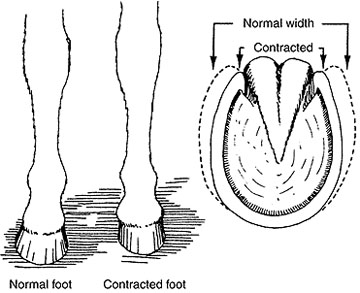
While walking, the horse with navicular disease tends to place its weight on the toe to avoid placing pressure on the heel area, which contains the inflamed navicular bone and bursa. Since the horse does not place weight on the heel, it takes longer to stop the stride. While standing the horse tends to shift its weight continuously. This relieves pressure, and thus pain, on the heel areas. Since the horse tends to place its weight on the toes during movement, the gait is very rough and sometimes gives the appearance of lameness in the shoulder. The horse is often lame after work, but the lameness may disappear with rest. Because there may be comparably poor circulation in the foot, the heels and adjacent hoof may become smaller and contract (Figure 2).
Diagnosis
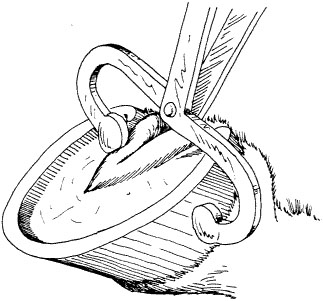
A veterinarian should be contacted when signs of lameness are noticed. Most veterinarians use hoof testers as an aid in the diagnosis of this condition. Applying pressure with hoof testers over the frog area produces pain, and the horse may flinch if the disease is present (Figure 3). The hindfeet should be tested with hoof testers to compare the reaction with that of the forefeet.
A locally injected anesthetic that temporarily blocks the nerve supply to the affected area will relieve the pain for a short period of time. In this way the veterinarian can determine whether or not navicular disease exists. If the horse was lame before the injection, and walks normally after the injection, it may be assumed that the lameness is located in the navicular area.
Treatment
Corrective shoeing is helpful. A bar placed across the heels aids in relieving the pressure on the heels. Rasping the quarters of the hoof wall or cutting grooves in the wall aids in relieving foot contraction. Rubber frog supports (properly applied) may be a superior method of restoring frog pressure. Cutting the nerves that supply the navicular area may be effective also, but can lead to several complications and therefore should be performed only when other approaches fail.
While the outlook for horses with navicular disease is unfavorable in most cases, the various methods of treatment discussed above may prove sufficiently effective to reduce the suffering of the horse and extend its useful service.